
Pectoralis Major Tear
The pectoralis major is a large muscle at the front of the chest, starting from two sections at both the sternum and the clavicle connected through tendons. Tears of the pectoralis major are extremely uncommon, occurring mostly through weightlifting during the eccentric of a movement such as bench or dumbbell press. This article will elaborate on the complications of a pectoralis major tear in addition to the anatomy behind the muscle.

Anatomy
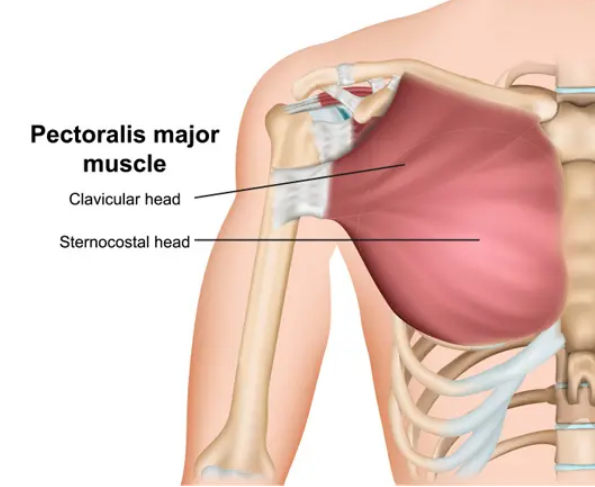
The pectoral muscles consist of the pectoralis minor, which is smaller and deep, and the pectoralis major, which is the superficial (outer) muscle that is much larger, therefore contributing a significant amount of strength during movements. The pectoralis major is made up of 2 heads, which are the sternal (breastbone) and clavicular heads. It assists in movement of the arm in both internal and external movement, rotation at the shoulder, and extension.
Mechanism of Injury
Pectoralis major ruptures or tears are becoming more prevalent, but are still a relatively uncommon injury. This type of injury predominantly affects men at ages 20-40 years old, and the majority of cases occur in weightlifters during chest workouts. The injury usually happens during an excessive strain on the fully contracted pectoral muscle, often resulting in the pectoralis tendon pulling away from the bone, a condition known as tendinous avulsion. There are classifications of this injury, identified by its severity and location.
Type I (Muscle contusion or sprain)
Type II (Partial Tear)
Type II (Complete Tear)
Location
A - Muscle Origin
B - Muscle Belly
C - Myotendinous Junction
D - Tendon avulsion off humerus (no bone)
E - Bony tendon avulsion off humerus
F - Tendinous rupture
Symptoms
Usually, the person will describe experiencing a sudden popping or tearing sensation while performing a chest exercise, such as a heavy weight-loaded bench or dumbbell press. This sensation is typically accompanied by pain and a feeling of weakness in the shoulder. It can also include:
Pain in your chest and upper arm
Weakness when arms are pushed out
Chest and arm bruising
Dimpling or pocket just above the armpit where the tear is located
Treatment from Doctors
During a physical examination from a doctor, they will feel the front of your chest, identifying the gap in the tendon from the tear. The palpation will draw the following conclusions:
Swelling and bruising of anterolateral chest wall and/or proximal arm
“Dropped nipple” sign – ipsilateral nipple will appear lower than the unaffected side due to medial retraction of muscle belly
Palpable defect and loss of anterior axillary contour – accentuated by resisted adduction
Further examinations and imaging to identify soft tissue of the pectoralis major include X-Rays, MRI scans, or Ultrasound imaging techniques.
Surgical Treatment
Repairing the tendon through surgery is usually performed within the first 2-3 weeks after the injury. After the procedure, scarring and shortening of the tendon and biceps muscle may occur, which potentially hinders the restoration of arm function through surgery. Although alternative options exist for patients wanting late surgical treatment for this injury, they tend to be more complicated and typically have lower success rates.
Nonsurgical Treatment
In order to regain full arm strength and function, surgery is necessary by the reattachment of the tendon to the bone. However, nonsurgical treatment may be considered to older and less active patients, in addition to those who are able to tolerate not having full arm function. For people who have medical complications putting them at higher risk for complications during surgery, nonsurgical treatment is also an option.
Nonsurgical treatment options aim to reduce pain and preserve arm function to the fullest extent possible. However, patients who have nonsurgical treatment will unfortunately experience a strength deficit and ongoing physical alterations due to the pectoralis rupture. Treatment recommendations include:
Rest - Avoid heavy lifting and any overhead activities to relieve pain and limit swelling. An arm sling is also highly recommended.
Nonsteroidal anti-inflammatory medications - Drugs such as ibuprofen and naproxen reduce pain and swelling.
Physical therapy - After the pain decreases, the doctor may recommend rehabilitation exercises to strengthen surrounding muscles in order to restore as much movement as possible.
Rehabilitation
Following surgery, the arm is placed in a sling to aid in wound healing. Patients commonly experience postoperative pain, which typically diminishes by the second day. Implementing multimodal pain management techniques has been demonstrated to enhance patient outcomes. Nighttime discomfort often presents the greatest challenge, yet employing multimodal pain strategies, warmth, and sleeping in an elevated position can alleviate this issue.
Several studies have indicated that patients can effectively rehabilitate their shoulder at home following surgery. Typically, patients follow a prescribed therapy routine and gradually reduce their reliance on the sling over the initial 8-12 weeks. Tendon integration typically takes around 4 months, with patients potentially resuming physical activities by the 5-6 month mark post-surgery. Consistent and continuous focus on increasing motion and strength can lead to further improvement for up to 1 year post-surgery.
Sources
“Pectoralis Major Rupture (PEC Tear).” Dr. Groh, 28 Apr. 2020, www.drgordongroh.com/orthopaedic-injuries-treatment/shoulder/pectoralis-major-rupture/.
“Pectoralis Major Rupture.” Physiopedia, www.physio-pedia.com/Pectoralis_Major_Rupture. Accessed 21 Feb. 2024.
“What Is a Pectoralis Major Muscle Tear?” WebMD, WebMD, 6 June 2022, www.webmd.com/fitness-exercise/pectoralis-major-muscle-tear-overview.